🦋TSH Normal Range for Women by Age: Pregnancy & Menopause
TSH 'normal' on your lab report may still be too high if you're pregnant or trying to conceive. Here's what TSH should be at every age and life stage for Indian women.
Dr. Anjali Mehta
Endocrinologist
TSH Normal Range for Women by Age: Pregnancy & Menopause Guide
Your thyroid panel came back and the only value flagged is TSH — Thyroid Stimulating Hormone. Your friend says anything under 5 is fine. Your lab marks 4.2 as "high." Your mother-in-law says thyroid problems cause weight gain. You are 28 and planning pregnancy — or 48 and dealing with hot flashes — and you have no idea what TSH you should actually aim for.
You are not alone. TSH is the most misunderstood number on a thyroid report in India. The "normal range" printed on lab reports is often wider than what endocrinologists prefer — especially for women of childbearing age, during pregnancy, and around menopause. This guide explains what TSH measures, age-specific and pregnancy-specific ranges, how TSH relates to T3 and T4, what high and low TSH mean for women, and when to see an endocrinologist.
For a full thyroid panel breakdown, see our thyroid test results guide.
What Is TSH — and Why Do Doctors Order It?
TSH is made by your pituitary gland (a small gland in your brain). It tells your thyroid gland (in your neck) how much T4 (thyroxine) and T3 (triiodothyronine) to produce.
Think of TSH as a thermostat in reverse:
| TSH Level | What Your Thyroid Is Doing |
|---|---|
| High TSH | Pituitary is shouting — thyroid is underactive (hypothyroidism) |
| Low TSH | Pituitary has gone quiet — thyroid is overactive (hyperthyroidism) |
| Normal TSH | Thyroid output matches your body's needs |
TSH is usually the first and most sensitive screening test for thyroid disorders. It changes before T4 falls in early hypothyroidism — which is why doctors trust it as the frontline marker.
Standard TSH Normal Range — and the Debate
Most Indian labs report TSH reference range as:
| Lab Reference (Common) | Interpretation |
|---|---|
| 0.4 – 4.5 mIU/L (or 0.4 – 5.0 mIU/L) | "Normal" on the printed report |
However, many endocrinologists — including guidelines used in pregnancy — prefer a tighter range for certain groups:
| Context | Preferred TSH Target |
|---|---|
| General healthy adults | 0.4 – 4.0 mIU/L (some use up to 2.5 as "optimal") |
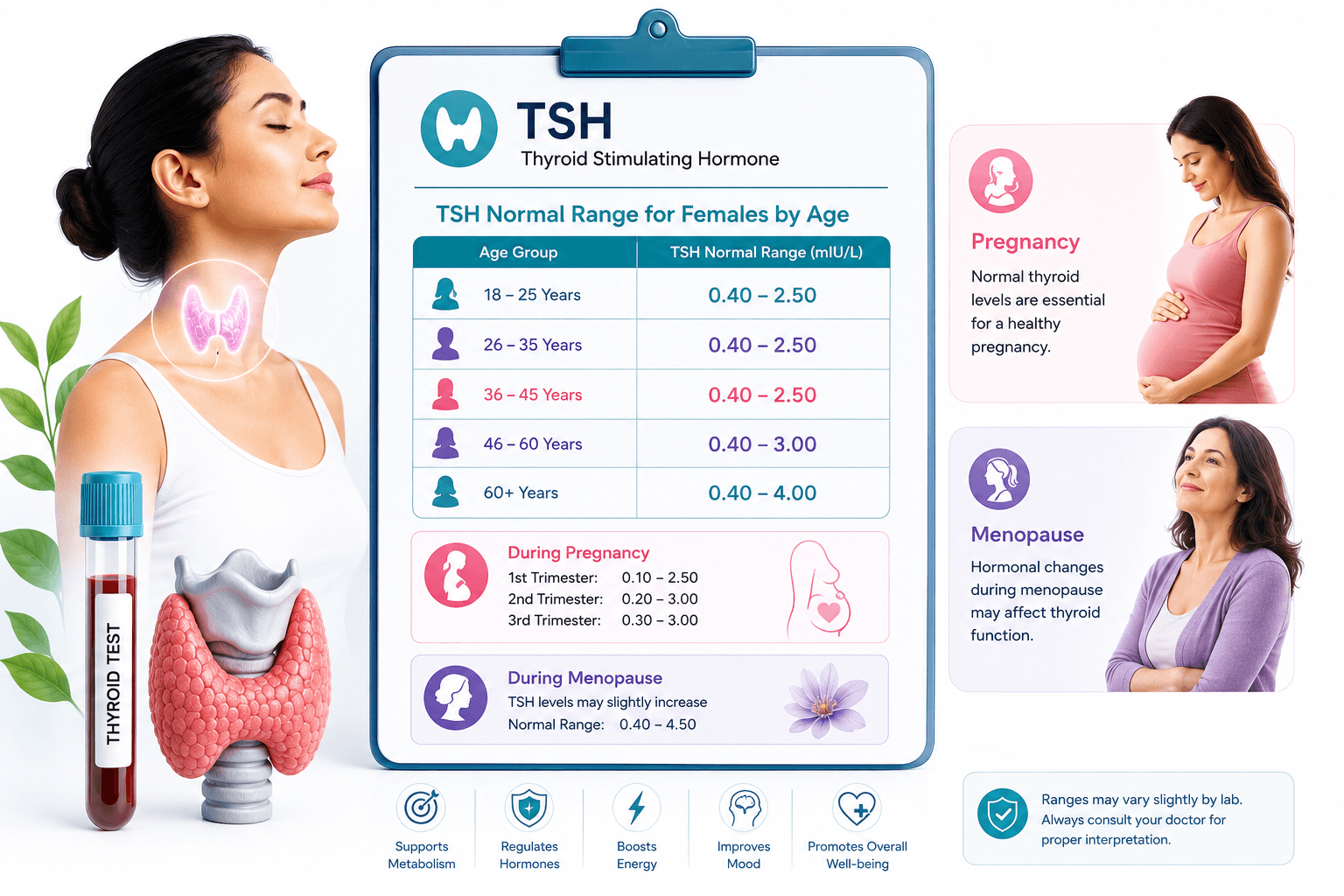
| Women planning pregnancy | < 2.5 mIU/L before conception |
| First trimester pregnancy | 0.1 – 2.5 mIU/L |
| Second trimester | 0.2 – 3.0 mIU/L |
| Third trimester | 0.3 – 3.5 mIU/L |
| On levothyroxine treatment | Individualised — often 0.5 – 2.5 mIU/L |
So a TSH of 4.2 mIU/L may be printed as "normal" on your lab report — but an endocrinologist may still want to treat it if you are pregnant, trying to conceive, or have symptoms + positive TPO antibodies.
This is not lab error. It is clinical context.
TSH Normal Range for Women by Age
Women are 5–8 times more likely than men to develop thyroid disease — especially Hashimoto's thyroiditis (autoimmune hypothyroidism). TSH also shifts naturally with age and life stage.
Women Aged 18–30 (Reproductive Years)
| TSH (mIU/L) | What It Usually Means |
|---|---|
| 0.4 – 2.5 | Ideal for most; target if planning pregnancy |
| 2.5 – 4.5 | Subclinical hypothyroidism zone — discuss if TPO positive, symptoms, or infertility |
| > 4.5 | Hypothyroidism likely — confirm with Free T4; treat especially if pregnant |
| < 0.4 | Possible hyperthyroidism — check Free T4 and Free T3 |
Indian context: Iodine intake varies by region. Iodised salt has reduced severe deficiency, but mild deficiency and autoimmune thyroid disease remain common. Routine TSH screening before marriage and pregnancy is increasingly recommended.
Women Aged 30–45 (Pregnancy & Postpartum)
Pregnancy dramatically changes thyroid hormone needs. hCG (pregnancy hormone) mildly suppresses TSH in the first trimester — so pregnancy-specific ranges are essential.
| Stage | TSH Target (ATA Guidelines) |
|---|---|
| Pre-conception | < 2.5 mIU/L |
| Trimester 1 | 0.1 – 2.5 mIU/L |
| Trimester 2 | 0.2 – 3.0 mIU/L |
| Trimester 3 | 0.3 – 3.5 mIU/L |
| Postpartum | Return to standard ranges by 6 months |
Why it matters: Untreated hypothyroidism in pregnancy increases risks of miscarriage, preterm birth, low birth weight, and can affect baby's brain development. Overtreated hyperthyroidism also carries risks.
Postpartum thyroiditis affects ~5–10% of women — often transient hyperthyroidism followed by hypothyroidism. Always retest at 6–12 weeks postpartum if TSH was abnormal.
Women Aged 45–55 (Perimenopause & Menopause)
Perimenopause overlaps with thyroid symptoms — fatigue, weight change, mood swings, irregular periods, heat intolerance. Many women discover thyroid disease during this decade.
| TSH (mIU/L) | Considerations |
|---|---|
| 0.4 – 4.0 | Generally acceptable |
| 2.5 – 4.5 with symptoms | Worth checking Free T4 and TPO antibodies |
| Rising trend over years | May indicate evolving Hashimoto's — even if still "in range" |
Hormone replacement therapy (HRT) for menopause does not usually distort TSH significantly, but oestrogen can raise TBG (thyroid binding globulin), making Total T4 look higher — another reason to rely on TSH and Free T4, not Total T4 alone.
Women Aged 55+ (Postmenopause)
TSH tends to rise slightly with age in healthy adults. Very strict "TSH must be under 2" targets are not applied to all elderly women — overtreatment can cause harm (atrial fibrillation, bone loss).
| Group | Practical Approach |
|---|---|
| Healthy, no symptoms | TSH 0.4 – 6.0 may be acceptable per some geriatric guidelines |
| On levothyroxine | Avoid TSH < 0.1 in elderly — cardiovascular and bone risk |
| TSH > 10 | Treatment generally recommended regardless of age |
TSH and the Full Thyroid Panel
TSH alone is a screening test. Complete evaluation often includes:
| Test | What It Shows |
|---|---|
| Free T4 (FT4) | Active circulating thyroxine — confirms hypothyroidism severity |
| Free T3 (FT3) | Active T3 — more relevant in hyperthyroidism |
| Anti-TPO antibodies | Hashimoto's autoimmune thyroiditis — very common in Indian women |
| Anti-Thyroglobulin | Additional autoimmune marker |
| Total T4 / Total T3 | Less useful alone — affected by pregnancy and oestrogen |
| Thyroid ultrasound | Goitre, nodules, thyroiditis pattern |
Common Patterns
| TSH | Free T4 | Diagnosis |
|---|---|---|
| High | Low | Overt hypothyroidism — treat |
| High | Normal | Subclinical hypothyroidism — watch or treat based on context |
| Low | High | Overt hyperthyroidism — treat |
| Low | Normal | Subclinical hyperthyroidism — monitor; common in early pregnancy |
| Normal | Normal | Euthyroid — thyroid function currently balanced |
High TSH in Women: Causes
Hashimoto's Thyroiditis (Most Common)
Autoimmune destruction of the thyroid. Often positive anti-TPO antibodies. Gradually rising TSH over months or years. More common in women with family history, other autoimmune diseases (type 1 diabetes, vitiligo), and after pregnancy.
Iodine Deficiency (Less Common Now)
Still seen in areas without consistent iodised salt use. Can cause goitre and hypothyroidism. Excess iodine (some seaweed supplements, contrast dye) can also trigger thyroid dysfunction.
After Thyroid Surgery or Radioiodine
Expected hypothyroidism — lifelong levothyroxine usually needed.
Medicines
- Lithium (psychiatry)
- Amiodarone (heart rhythm drug)
- Interferon, checkpoint inhibitors (cancer immunotherapy)
- High-dose biotin supplements — can falsely affect some immunoassay TSH/T4 tests (stop 48–72 hours before blood draw)
Pituitary Problems (Rare)
Very high TSH with low T4 can rarely mean pituitary resistance. Very low TSH with low T4 suggests central hypothyroidism from pituitary/hypothalamic disease — opposite pattern.
Low TSH in Women: Causes
Graves' Disease
Autoimmune hyperthyroidism. Symptoms: weight loss despite good appetite, palpitations, tremor, heat intolerance, bulging eyes (Graves' ophthalmopathy).
Toxic Multinodular Goitre
Common in iodine-sufficient areas with long-standing goitre.
Postpartum Thyroiditis (Transient)
Temporary low TSH phase — may not need aggressive treatment but needs monitoring.
Excess Thyroid Hormone Intake
Overtreatment with levothyroxine — TSH suppressed below 0.1; long-term bone and heart risks.
Early Pregnancy
hCG stimulates T4 production and lowers TSH in the first trimester — usually physiological, not Graves' disease.
Symptoms: Hypothyroid vs Hyperthyroid
| Hypothyroid (High TSH) | Hyperthyroid (Low TSH) |
|---|---|
| Fatigue, sluggishness | Anxiety, irritability |
| Weight gain | Weight loss |
| Cold intolerance | Heat intolerance, sweating |
| Constipation | Frequent stools |
| Dry skin, hair thinning | Fine tremor, palpitations |
| Heavy periods | Light or absent periods |
| Brain fog, depression | Insomnia |
| Swelling around eyes/face | Prominent eyes (Graves') |
Many symptoms overlap with stress, anaemia, vitamin D deficiency, and perimenopause — which is why blood tests, not symptoms alone, diagnose thyroid disease.
Subclinical Hypothyroidism: Treat or Wait?
Definition: TSH elevated (typically 4.5–10 mIU/L) with normal Free T4.
| Treat If… | Monitor If… |
|---|---|
| Pregnant or planning pregnancy | TSH 4–7, no symptoms, TPO negative |
| TPO antibodies positive | Mild elevation, young and well |
| Symptoms clearly thyroid-related | First abnormal test — repeat in 6–8 weeks |
| TSH > 10 mIU/L | Borderline with alternative explanation for symptoms |
| Goitre or fertility concerns |
Treatment is usually levothyroxine — one daily tablet on empty stomach, 30–60 minutes before breakfast. Coffee and calcium/iron supplements interfere with absorption — separate by 4 hours.
TSH Testing Tips for Accurate Results
- No fasting required for TSH — but morning draws are standard
- Consistent timing — TSH has minor diurnal variation
- Stop biotin 48–72 hours before if on high-dose supplements (>5 mg/day)
- Same lab for follow-ups — different assays vary slightly
- On levothyroxine? Take blood test before your morning dose (or 4+ hours after)
- Acute illness — defer routine thyroid testing until recovered
Pregnancy: A Special Case Every Woman Should Know
If you are pregnant or planning pregnancy:
- Request TSH + Free T4 — not TSH alone
- Ask about TPO antibody testing if TSH > 2.5
- Target trimester-specific TSH ranges (see table above)
- Increase levothyroxine dose by ~25–30% as soon as pregnancy is confirmed if already on treatment — do not wait for the next routine visit
- Every 4 weeks thyroid monitoring in first half of pregnancy, then at least once in later pregnancy
Untreated maternal hypothyroidism is preventable harm. Indian antenatal clinics increasingly screen TSH at the first visit — if yours did not, ask for it.
Menopause and Thyroid: Avoiding Confusion
Before attributing everything to "menopause" or "thyroid," get both evaluated:
- Perimenopause: irregular cycles, hot flashes, sleep disruption
- Hypothyroidism: constipation, cold intolerance, marked fatigue, high TSH
- Overlap: mood changes, weight gain, hair thinning
A simple TSH and Free T4 test clarifies the picture. Treating thyroid disease often improves symptoms you assumed were "just ageing."
When to Worry
Seek prompt endocrinology care if:
- TSH > 10 mIU/L with symptoms
- Low TSH + high Free T4 (overt hyperthyroidism) — palpitations, chest pain
- Pregnancy with TSH above trimester limit
- Neck swelling, difficulty swallowing, hoarse voice — large goitre or nodules
- Eye pain, vision changes, bulging eyes — Graves' ophthalmopathy emergency
- Very low TSH < 0.1 on treatment — overtreatment risk
Routine follow-up is fine for mild subclinical hypothyroidism — but do not ignore persistent abnormality on two separate tests 6–8 weeks apart.
Questions to Ask Your Endocrinologist
- "Is my TSH normal for my age — and am I pregnant or planning to be?"
- "Should I check Free T4 and anti-TPO antibodies?"
- "Is this subclinical hypothyroidism — do I need treatment now or monitoring?"
- "If I start levothyroxine, when do we retest?"
- "Could my medicines or biotin supplements affect this result?"
- "Does this explain my fatigue, weight change, or fertility concerns?"
How scanura Helps
Upload your thyroid report to scanura and see TSH, Free T3, Free T4, and antibody results explained in plain Hindi or English. Understand whether your values are borderline or critical for your life stage — and walk into your doctor's appointment with the right questions ready.
Key Takeaways
- TSH is a pituitary hormone that reflects thyroid function — high TSH means underactive thyroid; low TSH means overactive.
- Lab "normal" (up to 4.5–5.0 mIU/L) is not ideal for every woman — pregnancy and fertility targets are tighter (< 2.5 mIU/L).
- TSH ranges change by trimester in pregnancy — first trimester target is 0.1–2.5 mIU/L.
- Women of all ages are at higher risk for autoimmune thyroid disease — Hashimoto's is the most common cause of high TSH.
- Subclinical hypothyroidism (high TSH, normal T4) may need treatment if pregnant, symptomatic, or TPO antibody positive.
- Perimenopause symptoms overlap with thyroid symptoms — test before assuming "it's just hormones."
- Always confirm with Free T4 and repeat abnormal TSH before major treatment decisions.
- Levothyroxine works well but needs monitoring — take consistently and retest every 6–8 weeks after dose changes.
Disclaimer: This article is for educational purposes only. scanura does not provide medical diagnosis. Always consult your doctor for medical decisions.
Step-by-Step Guide
- 1
Know your life-stage target
General adults: 0.4–4.0 mIU/L. Planning pregnancy: under 2.5 mIU/L.
- 2
Use pregnancy-specific ranges
First trimester TSH should be 0.1–2.5 mIU/L — not the standard lab range.
- 3
Check Free T4 with abnormal TSH
TSH alone screens; Free T4 confirms overt vs subclinical thyroid disease.
- 4
Test anti-TPO antibodies
Positive TPO suggests Hashimoto's — more likely to need treatment.
- 5
Repeat before treating
Confirm abnormal TSH on a second test 6–8 weeks later unless pregnant.
- 6
Take levothyroxine correctly
Empty stomach, 30–60 minutes before food. Separate from calcium and iron by 4 hours.
📬 One health report guide, every week
Normal ranges, what your values mean, and what to ask your doctor — in plain language. Free, unsubscribe anytime.